
New headlines have brought up again, perhaps for the third time in 3-4 years, that not all adults over age 50 need a daily aspirin for cardiovascular prevention. The recent headlines arose, not out of new data, but out of a statement by an influential medical group (USPTF) that a daily aspirin was not needed for most health adults. There are nuances to these headlines and some patients with advanced heart disease need to further appreciate “primary” versus “secondary” prevention. Many do still need a daily aspirin and might be harmed by not interpreting the headlines correctly.
Who doesn’t not know the wisdom “take 2 aspirins and call me in the morning?” Although I am not sure who gets credit for this often repeated medical advice, the history of using aspirin related products is known to go back to the Greeks (Hippocrates), the Chinese, and the Phoenicians over 2,000 years ago. They recognized the power of the willow tree and its bark to relieve pain. In 1897, acetylsalylic acid (ASA or aspirin) was synthesized to maintain the benefits but reduce the stomach upset that often followed.
A forgotten figure is Lawrence Cravens, MD, practicing medicine in Glendale, California in 1950. He noticed that his patients having tonsillectomies and chewing aspirin gum had more bleeding. He jumped to the idea that he could possibly prevent heart attacks and strokes using a small daily dose of aspirin. He reported on treating 8,000 patients in his practice in this manner with a very low rate of events. He also experimented on himself and found that 12 aspirin a day gave him nosebleeds within 5 days. Overall, he showed the benefit and the risks of aspirin that are in the headlines now.
What is Secondary Prevention?
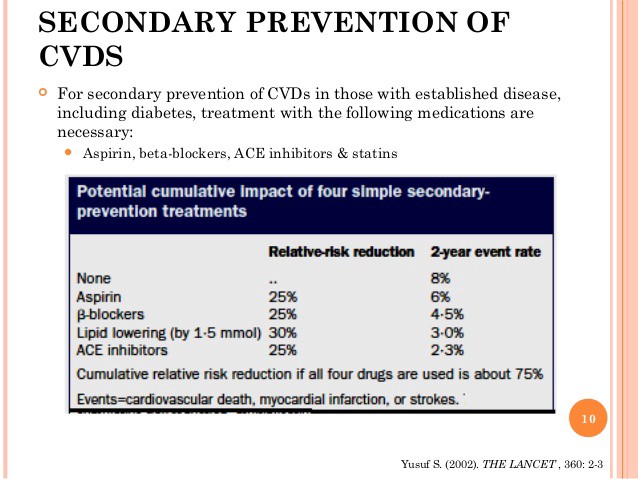
Secondary prevention of cardiovascular disease relates to aspirin and other agents after the diagnosis of an event. Patients after a heart attack, stroke, TIA (mini-stroke), heart or leg bypass surgery, stent procedure, or known artery narrowing from and angiogram all are approached as secondary prevention, the deed is done and the disease is known. There have been NO changes in terms of recommendations for aspirin use in those that can tolerate it in patients like those listed above.
What is Primary Prevention?
Primary prevention is the attempt to lower the risk of future events like strokes, heart attacks, and heart deaths in individuals not yet known to have disease or an event. Suggestions for taking a low-dose daily aspirin has been quite common for this purpose and millions of people in the USA alone practice this habit.
What are the ACC Guidelines About Aspirin?
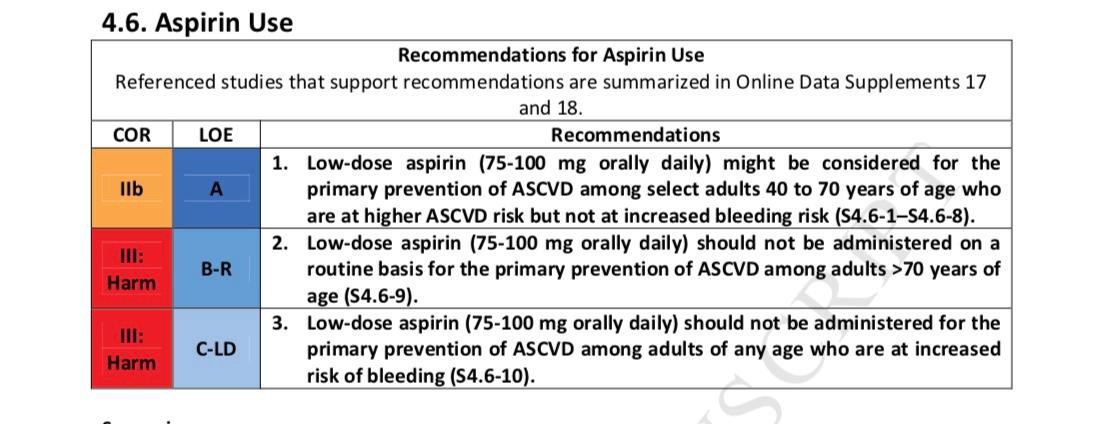
The American College of Cardiology (ACC) along with the American Heart Association (AHA) released new guidelines many health care practitioners look to for advice. Earlier this year these guidelines were updated and they addressed aspirin. The recommendations for aspirin for primary prevention and were scaled way back as shown here.
Why Are There More Headlines Now?
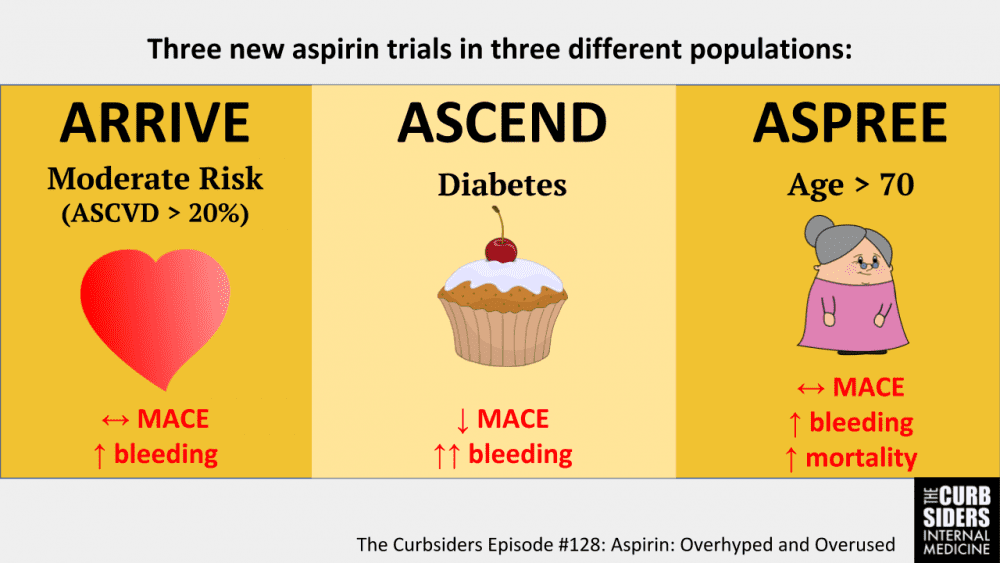
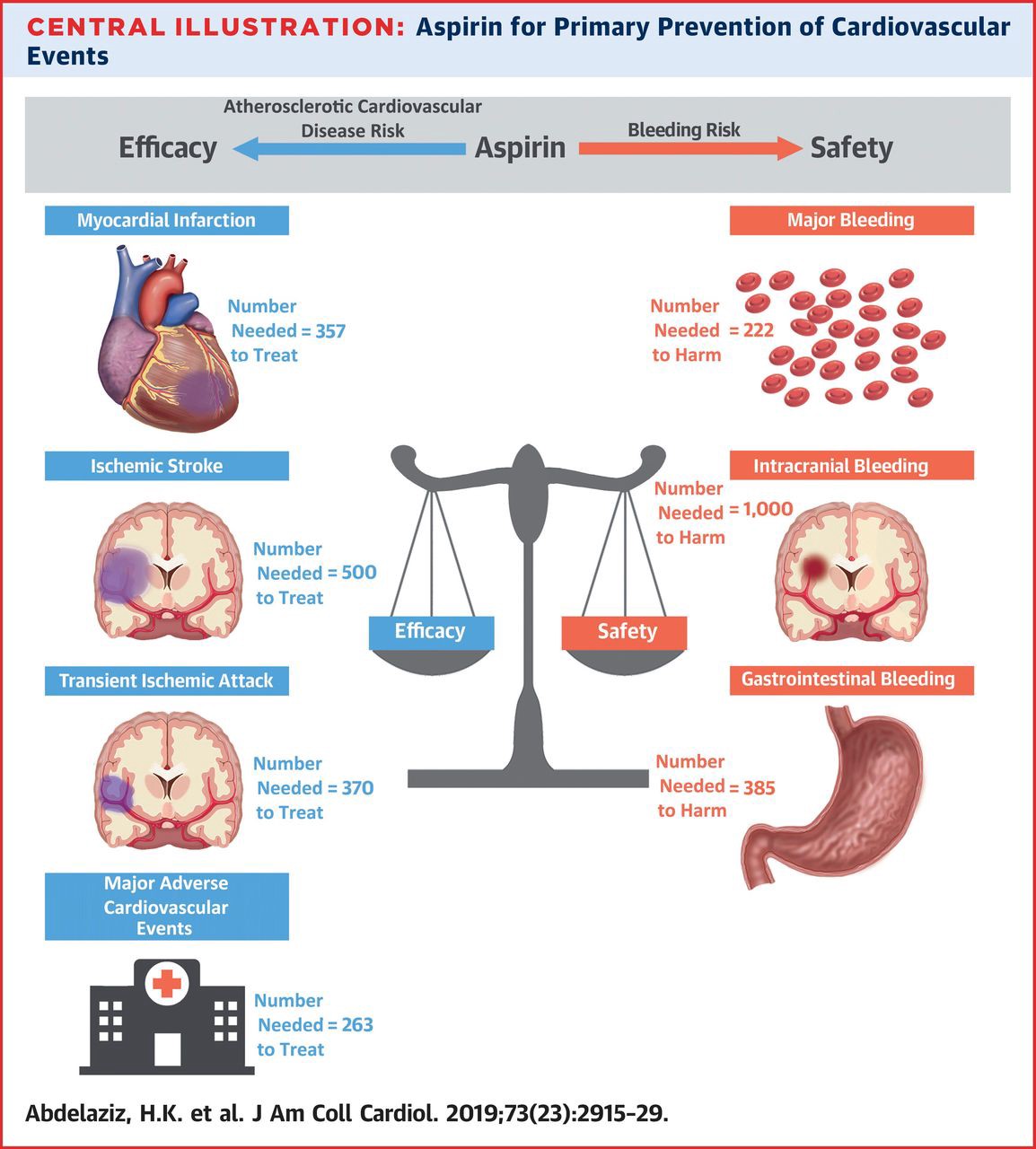
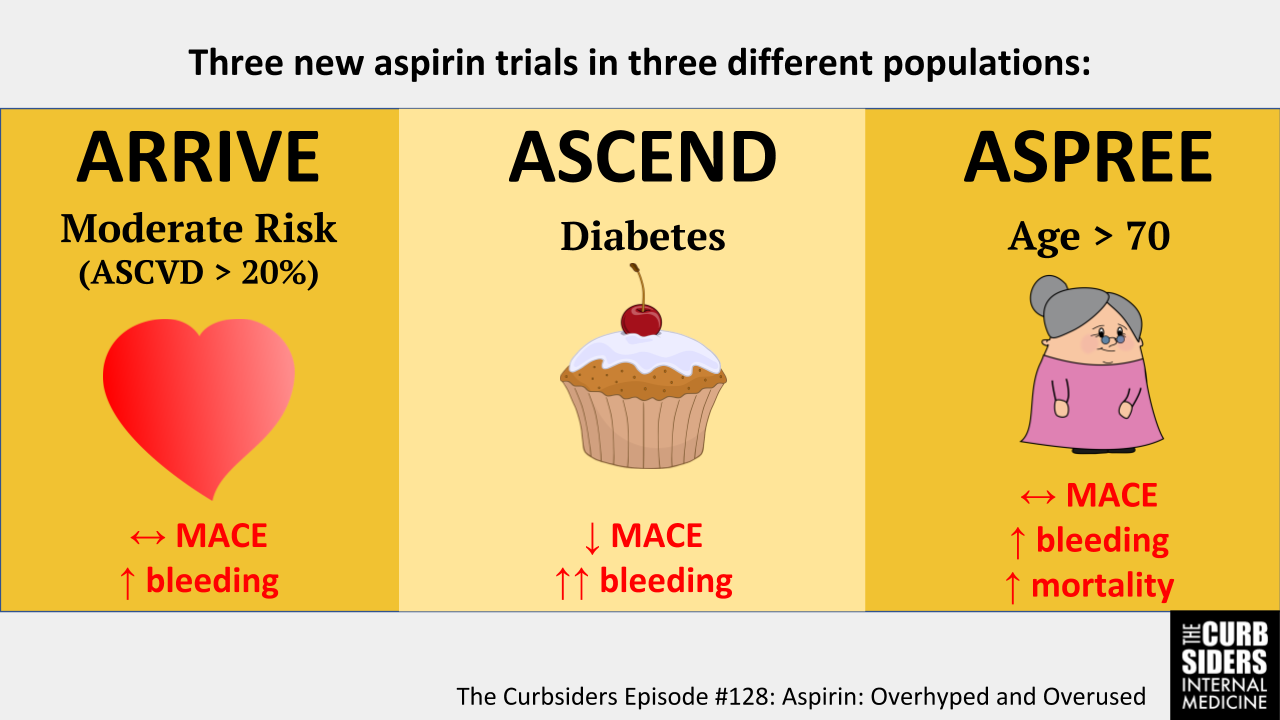
In late 2018 there were 3 new large randomized trials published testing the idea that a daily low-dose aspirin might reduce cardiovascular events. In total, nearly 50,000 subjects were including in these studies followed for 5–7 years. The findings were quite consistent across the trials even though the age and health of the study subjects were somewhat different in all 3. Overall, any benefit from a daily aspirin was offset by an increased risk of bleeding, just as Dr. Cravens showed over 60 years ago. The term major adverse cardiac events or MACE (stroke, heart attack, death) was used in the studies as an end point and there was no convincing drop in this measurement. Overall, there are now over 165,00 patients in randomized trials of aspirin for primary prevention, including these 3 new trials, and no convincing benefit without harm has been shown.
What To Do?
If you have had a prior cardiovascular event (heart attack, stroke, bypass surgery) you probably should be on aspirin daily and if you have had a recent heart stent, you have to be on one. Talk to your treating doctor or schedule a consult at the Kahn Center.
If you fall in the primary prevention group, you probably should not take one. I do not. If you are uncertain, there is an online calculator you can use called Aspirin Guide. A final group to consider is the many people that have had a coronary artery calcium CT scan (CACS) that is not a zero score. In general, the advice to recommend a daily low dose aspirin for those with a CACS over 100 is reasonable.