
Why Get a Heart CT Scan?
The introduction of a simple, inexpensive, and safe screening test for silent CAD over a decade ago (CACS) should have been a complete gamechanger in the approach to “winning the war” against CAD. The CACS was recommended as early as 2005 by the SHAPE society. The CACS does not involve injecting any chemicals or contrast, is painless, takes under a minute, and is widely available at hospitals worldwide. Unfortunately, the introduction of the CACS, sometimes called the “heart’s mammogram”, has been very slow and many have suffered heart attacks and deaths that could have been predicted months to years before their tragic events. The tide seems to be changing however as the cost of the CACS has dropped as low as $50 in some hospitals.
Updated practice guidelines have incorporated the exam into patient evaluation, and the press has highlighted examples of how the CACS has changed habits and even saved lives. There are useful summaries about the CACS exam that are worth reviewing.
In a powerful recent study, asymptomatic people with a CACS >300 had the same risk of heart events as a group with established heart disease like prior heart attack or stents. It is common in my clinic to meet patients with this degree of heart calcification and they must be treated aggressively.
What Do I Do With the Results?
Although getting the scan done is an important step, usually necessitating a prescription from a health care practitioner, the proper path after the CACS is less clear. There are simply not enough definite and prospective research studies. I have read thousands of the CACS exams, have ordered thousands more, and have managed patients from around the world for over 20 years who have an abnormal CACS. Their question, and maybe yours too, is always “what do I do about the CACS?” At the Kahn Center for Cardiac Longevity we take certain steps in the evaluation and treatment of patients with abnormal CACS and some of those protocols are listed here.
Step 1. Calculate Your Risk of Heart and Stroke Events After Your CACS
In a publication of the American College of Cardiology, two valuable statements are made that I am sharing here.
CAC progression is associated with a higher risk for myocardial infarction (heart attack) and all-cause mortality. CACS increase by about 20-25% per year and about 20% of subjects with a CACS = 0 progress to CACS >0 in 5 years and increases markedly with age, but less so in women. The best CAD prognosis is in patients with a CACS = 0 at baseline and 5 years later. ‘Double zero’ was associated with a 10-year risk of 1.4% followed by new-onset CAC at 5 years of 1.8%. After an initial abnormal CACS, a repeat scan after 5 years appears to be of additional value except for those with a double-zero or already high risk because of a CACS >400. An more recent alternative to a follow up CACS at the Kahn Center is choosing the option of a coronary CT angiogram (CCTA) read by artificial intelligence (AI) algorithms called a Cleerly Health CCTA. This is usually a cash pay option that offers incredible precision about the type and amount of coronary plaque. It is not a good option if there is a serious iodine contrast allergy or kidney disease.
MESA Risk Score
A valuable and useful tool in support of CACS for risk assessment was developed in the MESA study, in which CACS was incorporated into a model using 10-year follow-up data of any coronary heart disease (CAD) outcome. The MESA risk score is available online and incorporates age 45-85 years. It provides 10-year CHD risk with and without the CACS.
AstroCHARM Calculator
A more update risk calculator you may want to use is called Astro-CHARM and is available online for free. You will have to know your blood pressure and some laboratory results. The Astronaut Cardiovascular Health and Risk Modification (Astro-CHARM) calculator is a tool that incorporates traditional risk factor information with coronary artery calcium (CAC) score results to provide an individual’s estimated 10-year risk of atherosclerotic disease (ASCVD) events, including fatal or non-fatal heart attack or stroke. It is intended for use in younger individuals (ages 40-65) without a prior history of ASCVD. The Astro-CHARM was developed using data from three large, population-based cohorts (the Multi-Ethnic Study of Atherosclerosis, Dallas Heart Study, and Prospective Army Coronary Calcium Project), and validated in a fourth cohort (the Framingham Heart Study).
I find calculating the Astro-CHARM with patients reassures them that a heart attack, stroke and death are not likely even with a high CACS. For example, if the calculator predicts a 5% risk of a heart attack, fatal or not, or a stroke over 10 years, that is a 95% chance of not having those events. If you assess that yearly, it is a 99.5% chance each year that a bad outcome will not occur in this example. It also helps discuss what therapies might be used versus the potential side effects. It is challenging to predict that a therapy will lower a 0.5% yearly risk to an even lower level particularly if side effects are common. Of course, the risk of diet and exercise changes discussed below is essentially absent so that is always the thrust of the long-term plan.
Step 2. Why Do I Have an Abnormal CACS?
This is a crucial question that must involve assessing any smoking history, fitness regimen, current diet, stress level, sleep and snoring history, weight, blood pressure, and routine laboratories. If there is loud snoring or apnea at night, a sleep study, often done in your own bed, is recommended. There are advanced labs I order on patients at the Kahn Center that include:
Advanced lipid profile (NMR Lipoprofile): Rather than giving you a calculated LDL cholesterol level, advanced panels measure LDL particle number and size, which are more predictive of future heart and stroke events. Two people with the same cholesterol levels can have widely different particle and size measurements, making for very different risks.
Hs-CRP: The middle of the word inflammation is flame and it means the immune system is turned on and increasing the risk of atherosclerosis, heart attack, stroke and even other conditions like cancer and dementia. Bloodwork for the hs-CRP and additional measures like MPO and Lp-Pla2 are recommended.
Lipoprotein (a): This is a genetic form of cholesterol that’s elevated in about 20% of those tested. It’s rarely drawn even though hundreds of research studies indicate that if it’s high, the risk of heart attack and stroke skyrocket. It runs high in many families that have been decimated by heart disease.
Homocysteine: This amino acid is produced by a process called methylation. It can injure arteries when elevated. It may be due to a genetic defect in the MTHFR gene, which is easily measured. It can be treated with methylated B-complex vitamins.
Genetics: More and more we are offering genetic panels that include at a minimum blood or cheek swab samples for the 9p21 and ApoE gene. Although there is no way to change the gene, inheriting abnormal versions of these genes is common and a powerful factor in developing a high CACS.
Step 3. Do I Need a Stress Test?
I generally do not order the CACS when a patient has symptoms of classic angina, that is, pressure or tightness on exertion relieved quickly by rest. After a full evaluation, the decision is usually a stress test, a coronary CT angiogram (CCTA) with contrast injections and flow measurements (FFR Heartflow), or directly to an invasive cardiac catheterization.
In the much larger population without angina but interested in the CACS for prevention, a stress test has been recommended even in the absence of any chest symptoms if the CACS is >300-400. This can be a routine treadmill test, a stress echo treadmill test, or rarely in my practice, a stress nuclear radioactive treadmill test. I reserve the nuclear examinations for obese patients and those with an EKG finding called a left bundle branch block and usually a “chemical” stress test is selected. If you score is over 400, I suggest you consider a stress test, usually a stress echo examination. If it is very abnormal for signs of reduced blood flow to the heart, a cardiology consultation, initiation of medical and lifestyle therapy, and an invasive cardiac catheterization or CCTA is usually appropriate.
There are some patients with low CACS results but still with symptoms that are concerning for angina pectoris. It is rare, but possible, to have a badly blocked heart artery with a low or even a zero CACS due to “soft” plaque. I always perform a complete history and physical examination to assess any chest symptoms and may order a CCTA if their is angina pectoris.
Step 4. Do I Need a Heart Catheterization (angiogram)?
There are differences of practice If your CACS returns at a very high score (e.g. >1000) even if you have no symptoms. Some cardiologists recommend an invasive cardiac catheterization as described in a recent media article. I have performed cardiac catheterization on dozens of people with scores over 1,000 (one as high as 6,000) and often found only mild plaque or one totally blocked artery that was treated with medication and lifestyle. Rarely, the blockages found in an asymptomatic person is so advanced, often coupled with a markedly abnormal stress test, that a discussion about a coronary stent or even coronary artery bypass grafting is appropriate. Overall, this is rare. In my clinic practice, I usually first recommend a stress test rather than a cardiac catheterization in patients without any symptoms or other high-risk features. An individualized approach is recommended when you discuss this with your cardiologist. With improved CT scanners, CCTA is less expensive, safer, and much less radiation than a cardiac catheterization. It is the preferred approach. My colleagues at Cleerly Health relate they can analyze a CCTA with a high CACS using AI interpretation successfully.
Step 5. Do I Need Lifelong Medication?
One of the strongest arguments to have a CACS is that if you have a zero score and have no symptoms, there is growing agreement that there is not need for a daily aspirin or a statin cholesterol lowering medication. Lifestyle discussed below emphasizing a healthy diet is always a recommendation. A statement by a joint group of the American Heart Association and the American College of Cardiology in late 2018 incorporated the concept that a CACS before starting a statin prescription was acceptable and avoiding medication after a Zero CACS was often preferable. The same is true for daily aspiring.
If the CACS is over 100, there are recommendations that incorporate routine low dose aspirin (81 mg) and statin medication daily. An example of the “standard” approach to an abnormal CACS is outlined in a recent medical article. A study recently published looked at a database of 13, 644 patients studied for heart artery disease by a coronary calcium CT scan and followed for over 9 years. The group was also analyzed as to whether they were on a statin medication to lower their cholesterol. When the CACS calculated as abnormal at 100-400, or over 400, treatment with a statin was associated with a lower risk of bad outcomes. In fact, when the calcium score was over 100, only 12 patients needed to receive a statin to prevent one event like a heart attack, stroke, or death.
Step 6. What Can I do to Reverse Atherosclerosis?
In my clinic, a major emphasis after an abnormal CACS is education on the research indicating that CAD can be halted and reversed, even if it requires significant lifestyle changes. The details follow here.
I was taught in medical school that CAD, or the blockages that can choke off blood flow to the heart, progresses from minor “streaks” in youth, to visible plaques young adulthood, and on to complicated plaques and major problems later in life. During my training the arrow always pointed towards heart disease advancing and never reversing. This is just not true! Indeed, for nearly 3 decades it has been known that just as arteries can worsen with time, they can also improve rapidly. Some of the measures to achieve this are presented here.
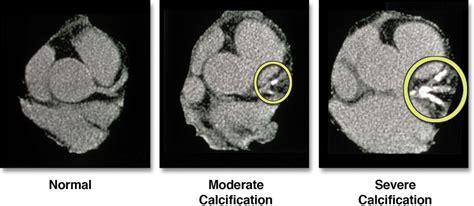
Statin Medication
While reversal of clogged heart arteries has been shown before, most of the studies actually look at other endpoints like risk of heart attack and even survival in patients with calcified arteries treated with statins. A study just published looked at a database of 13, 644 patients studied for heart artery disease by a coronary calcium CT scan and followed for over 9 years. The group was also analyzed as to whether they were on a statin medication to lower their cholesterol. As the picture above demonstrates, when the score, a measurement of how much calcium was in the heart arteries, was calculated as abnormal at 100–400, or over 400, being treated with a statin was associated with a lower risk of bad outcomes. In fact, when the calcium score was over 100, only 12 patients needed to receive a statin to prevent one event like a heart attack, stroke, or death.
Plant-Based Nutrition
This one-way street towards worsening was shown to be incorrect in 1990 by Dean Ornish, M.D. He prescribed a plant-based diet without added fats to patients with proven heart blockages. He also recommended walking, social support and stress management to help their hearts. He demonstrated that the patients who adhered to his “lifestyle program” felt better and showed reductions in the amount of narrowing in their arteries. Dr. Ornish followed his patients for longer periods of time and with further testing and showed even more improvements, avoidance of hospitalizations, and reduced costs. Since those first reports, the data that heart disease can be reversed by intensive lifestyle changes emphasizing a plant-based diet low in added fats has become so robust that the Ornish Lifestyle program was recognized by Medicare in 2010 for reimbursement as a therapy of CAD. Another similar program, based out of the Pritikin Longevity Center in southern Florida, received the same Medicare designation for intensive therapy and reversal of heart disease with dietary therapy.
Because both the work done by Dr. Ornish, and the original site of the Pritikin Center was in California, it could be argued that the plant based dietary reversal of heart disease is only a West coast thing. Fortunately, a similar research program at the Cleveland Clinic Foundation led by Dr. Caldwell Esselstyn monitoring patients with advanced heart disease who converted to totally plant based diets without added oils identified the same types of clinical improvements with documents shrinking and reversal of heart blockages.
Extra Virgin Olive Oil (EVOO): Heart disease reversal studes have generally avoided EVOO while the Mediterannean diet features EVOO in place of animal fats like butter, tallow and lard. A large randomized study in 1,002 CAD patients in Spain called CORDIOPREV has been studying the impact of a diet high in EVOO versus a low oil version. The results have been stunning favoring the EVOO group. When measurements of carotid plaque were made, the EVOO rich diet won out over the low EVOO diet and were published. When the 7 year results were published there was an important advantage to the high EVOO group in avoiding cardiac outcomes. The highest polyphenol EVOO I am aware of is ice pressed Rallis Olive oil at www.rallisoliveoil.com using discount code Drjoelkahn.
Aged Garlic
Although all whole plant foods can contribute to heart disease reversal, special mention is earned by a few. The ability of garlic to lower blood pressure, cholesterol, and blood clotting has been recognized for some time. There have actually been a surprising number of studies testing the ability of aged garlic extract to halt heart disease progression. For example, in a study published in early 2016 that used baseline and follow-up CT angiograms of heart arteries, aged garlic extract reduced areas of plaque in heart arteries at the one-year follow-up. In addition to the sulfur content of garlic, onions also provide a source of sulfur in the diet that may be crucial for maintaining optimal amounts of antioxidants. The aged garlic used in the study is available online (https://shop.drjoelkahn.com/kyolicr-aged-garlic-extracttm-one-per-day.html).
Pomegranate
Pomegranate juice and seeds both have powerful antioxidant properties that may improve the function of HDL cholesterol. This protective cholesterol may boost the reverse cholesterol transport, or “vacuum cleaner” function in arteries, that may reverse CAD. In studies of mice, pomegranates can reduce atherosclerosis although translating animal research to human health can be misleading. In humans with increased stress at risk for CAD, pomegranates can reduce evidence of arterial damage. In another study using pomegranate juice for three years, the degree of narrowing in carotid arteries of five study subjects was reduced. Pomegranate extracts are available online (https://shop.drjoelkahn.com/pomegranate-complete-30-softgels.html).
Chelation etc.
Beyond diet, there may be other methods supported by scientific studies to reverse atherosclerosis. Over 60 years ago some data surfaced that chelation therapy (latin for claw) using disodium ethylene diamine tetraacetic acid or EDTA could reverse heart artery disease. It took many decades but the Trial to Assess Chelation Therapy (TACT) was published in 2013 and demonstrated an improvement in outcomes in post-myocardial infarction (MI) patients following IV EDTA versus a placebo. The TACT showed a particularly large reduction in CVD events and all-cause mortality in the subgroup of patients with diabetes. An ongoing TACT2, limited to patients with heart disease and diabetic mellitus type 2, is further examining this unique therapy in the hope that it may enter the armamentarium to reduce the atherosclerotic risk of their diabetic patients.
There is an interesting oral agent containing EDTA and additional agents that has data for lowering the calcification of coronary arteries in peer reviewed data. Other components of the novel combination may attack the mechanism of calcification and lead to reversal of plaque. I have successfully used NanobacTX in heart patients in my clinic.
Other Nutraceuticals
Other promising therapies for the reversal of atherosclerosis using nutraceutical therapies have appeared. In a recently published randomized study from China, 76 patients with carotid atherosclerosis were treated with either nattokinase (NK) 6,000 FU or simvastatin 20 mg (). In both groups cholesterol fell, and in the NK group HDL rose, but reversal of atherosclerosis over 26 weeks was profound with NK and plaque volume fell by 37%.
In another study from China in 2009, 60 patients with carotid plaque were divided aspirin and atorvaststatin. Half also got lumbrokinase, 2 capsules three times a day for 6 months. Lumbrokinase is an enzyme extracted from earthworms. Measurements of CIMT were lower in the group treated with lumbrokinase as were measures of cholesterol fractions and platelet aggregation. The use of lumbrokinase was safe in this small study. Nattokinase is available online (https://shop.drjoelkahn.com/nattokinase-nsk-sdr.html).
Another agent, bergamot, was studied in patients with atherosclerosis over 6 months without randomization. Lipid fractions improved as anticipated during therapy with bergamot and there was a stunning decrease in the CIMT from 1.2 cm to 0.9 cm. The product is available (https://shop.drjoelkahn.com/bergamet-mega-o.html).
Vitamin E has 8 forms and 4 of them are classified as tocotrienols with properties far more favorable than the more common tocopherols. In a study of 50 patients with carotid disease, half were treated with a source of gamma tocotrienol from palm oil. Over 18 months of therapy, regression of plaque was seen in 7 of the 25 patients treated with the vitamin E preparation while in the control group none regressed and 10 showed worsening. The product is available online (https://shop.drjoelkahn.com/annatto-etm-300.html).
A promising combination therapy has been reported to promote the reversal of carotid atherosclerosis. The study combined pycnogenol with centella asiatica and followed 391 patients with ultrasound measurements of plaque for over 4 years in a randomized trial. The progression of plaque over time was least in the patients treated with the combination nutraceutical and there was reduction in the number of angina episodes and myocardial infarctions in the treated cohort. The product is available online (https://shop.drjoelkahn.com/arterial-protect.html).
A study of a green algae extract in a capsule given twice a day for 2 months was reported that examined the impact on the “lipid rich necrtoic core” of carotid plaque using MRA to assess the arteries before and after. The preliminary findings of this ongoing study in China indicate significant decreases of 50% or more in this measure of disease and provides a hopeful avenue of therapy by emphasizing the endothelium and its glycocalyx. The product is available online (https://shop.drjoelkahn.com/arterosil-hpr-60-vegan-capsules.html).
Berberine is a natural agents from a variety of plants like the barberry that has human data to lower blood sugar and blood cholesterol. A recent small study in humans showed it also reversed carotid plaque measured by ultrasound within just a few months. Berberine is available online (https://shop.drjoelkahn.com/berberine-1000-mg-60-capsules.html).
Tongxinluo is a combination product developed and researched in China that has been tested in animal models and found to reverse atherosclerosis. It has some unusual components like those derived from scorpions! Exotic for sure. In a recent paper in over 1,000 human subjects, TXL as it is called, reversed carotid plaque and prevented cardiac events, quite an impressive finding. It is possible to buy TXL online and it is shipped from China.
Cyclodextrin (RemCHOL) is a molecular ring of 7 glucose molecules that can trap a cholesterol molecule in its inner circle and appears to be able to remove cholesterol from damaged artery walls and organs (reverse cholesterol transport or RCT). It has been approved for use in a rare childhood disease called Nieman-Pick Disease and is given intravenously. A rectal application is necessary for more routine use as an oral route leads to degradation in the intestinal tract due to digestive enzymes. Although a randomized clinical trial is not available, the safety has been proven and it is a promising area of care and research available online (www.cavadexusa.com using discount code DRJKMD).
Licorice extracts, or DGL, reduce blood pressure and cholesterol levels. In a recent study in 110 subjects, taking DLG for a year resulted in lower blood pressure, lower cholesterol, and decreased carotid plaque measurements made by CIMT analysis as is used at the Kahn Center. DGL is available online as a chewable tablet (https://shop.drjoelkahn.com/dgl-synergy-90-chewable-tablets.html).
Vitamin K2 is difficult to source in a plant-based diet unless natto beans are added to the diet. There has been much hope that the impact on coronary calcification would facilitate using vitamin K2 for plaque reversal. To date, the studies are hopeful but unfulfilled. In a randomzed study of very high dose vitamin K2 on the progression of valvular aortic stenosis (not CAD), there was no slowing of the aortic valve calcification over 24 months. Somewhat hidden in the study data was a comment that CACS measurements were also made before and after the 2 years and there was no reversal of the CACS although there was a non-statistical trend to slower progression of the CACS. No measures of soft plaque were made.
EXERCISE
HIIT: While it is intuitive that exercise might reverse atherosclerosis, a new report indicates that high-intensity interval training or HIIT can reduce plaque volume in heart arteries. This study indicates that high-intensity interval training counteracts atherosclerotic coronary disease progression and reduces atheroma volume in residual coronary atheromatous plaques following stent placement.
Endurance training: A shocking study was just published analyzing the amount of soft and non-calcified coronary artery plaque burden in middle aged men who were grouped in lifelong endurance athletes, later in life endurance athletes, and average exercisers. All groups were fit and low risk. Not only was their more calcified plaque (CACS) in the lifelong endurance athletes, there was more non-calcified and soft plaque, including in proximal important heart arteries, in lifelong endurance athletes. This special group should be offered at least a CACS and not ignore the possibility of CAD.
CONCLUSIONS
Advances in the detection, prevention and reversal of atherosclerosis are sorely needed but there are many pathways of treatment backed by science available right now. These studies give hope that even for patients with advanced disease, nutrition, exercise, and nutraceutical therapies can improve their quality and quantity of life.